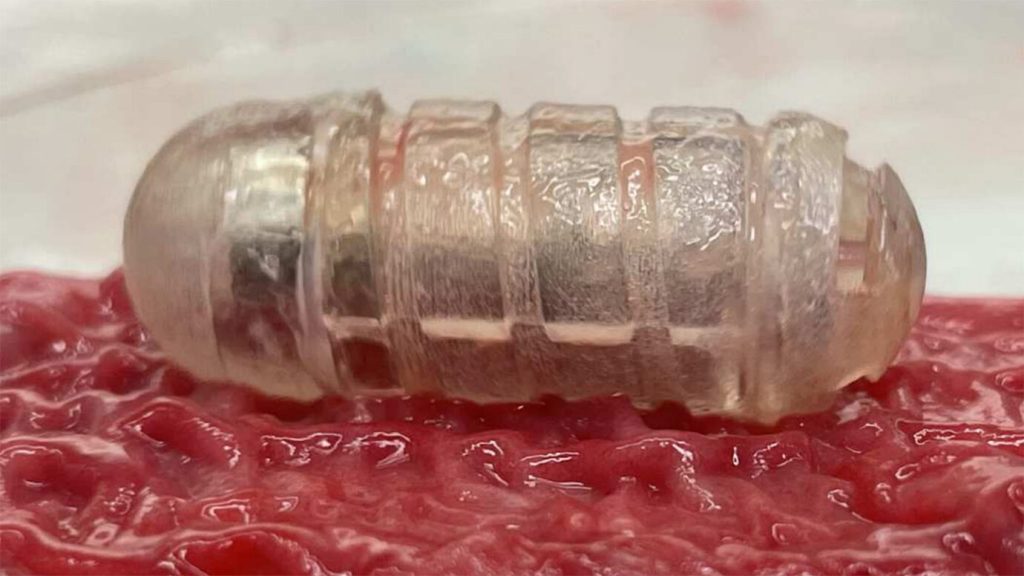
A mucus-wicking robotic pill may offer a new way to deliver meds.
The multivitamin-sized device houses a motor and a cargo hold for drugs, including ones that are typically given via injections or intravenously, such as insulin and some antibiotics. If people could take such drugs orally, they could potentially avoid daily shots or a hospital stay, which would be “a huge game changer,” says MIT biomedical engineer Shriya Srinivasan.
But drugs that enter the body via the mouth face a tough journey. They encounter churning stomach acid, raging digestive enzymes and sticky slicks of mucus in the gut. Intestinal mucus “sort of acts like Jell-O,” Srinivasan says. The goo can trap drug particles, preventing them from entering the bloodstream.
The new device, dubbed RoboCap, whisks away this problem. The pill uses surface grooves, studs and torpedo-inspired fins to scrub away intestinal mucus like a miniature brush whirling inside a bottle. In experiments in pigs, RoboCap tunneled through mucus lining the walls of the small intestine, depositing insulin or the IV antibiotic vancomycin along the way, Srinivasan and colleagues report September 28 in Science Robotics. After churning for about 35 minutes, the pill continued its trip through the gut and eventually out of the body.
RoboCap is the latest pill-like gadget made to be swallowed. In 2019, some of the same researchers who developed RoboCap debuted a different device — one that injects drugs by pricking the inside of the stomach (SN: 2/7/19). That pea-sized injector was not designed to work in the small intestine, where some drugs are most easily absorbed. The RoboCap may also be able to deliver larger drug payloads, Srinivasan says.
Great scientists become immortalized in various ways.
Some through names for obscure units of measurement (à la Hertz, Faraday and Curie). Others in elements on the periodic table (Mendeleev, Seaborg, Bohr, among many others). A few become household names symbolizing genius — like Newton in centuries past and nowadays, Einstein. But only one has been honored on millions and millions of cartons of milk: the French chemist, biologist and evangelist for experimental science Louis Pasteur.
Pasteur was born 200 years ago this December, the most significant scientist birthday bicentennial since Charles Darwin’s in 2009. And Pasteur ranked behind only Darwin among the most exceptional biological scientists of the 19th century.
Pasteur not only made milk safe to drink, but also rescued the beer and wine industry. He established the germ theory of disease, saved the French silkworm population, confronted the scourges of anthrax and rabies, and transformed the curiosity of vaccination against smallpox into a general strategy for treating and preventing human diseases. He invented microbiology and established the foundations for immunology. Had he been alive after 1901, when Nobel Prizes were first awarded, he would have deserved one every year for a decade. No other single scientist demonstrated more dramatically the benefit of science for humankind.
He was not, however, exactly a saint. A Pasteur biographer, Hilaire Cuny, called him “a mass of contradictions.” Pasteur was ambitious and opportunistic, sometimes arrogant and narrow-minded, immodest, undiplomatic and uncompromising. In the scientific controversies he engaged in (and there were many), he was pugnacious and belligerent. He did not suffer criticism silently and was often acerbic in his responses. To his laboratory assistants, he was demanding, dictatorial and aloof. Despite his revolutionary spirit in pursuing science, in political and social matters, he was conformist and deferential to authority.
And yet he was a tireless worker, motivated by service to humankind, faithful to his family and unwaveringly honest. He was devoted to truth, and therefore also to science. In his youth, Pasteur did not especially excel as a student. His interests inclined toward art rather than science, and he did display exceptional skill at drawing and painting. But in light of career considerations (his father wanted him to be a scholar), Pasteur abandoned art for science and so applied to the prestigious École Normale Supérieure in Paris for advanced education. He finished 15th in the competitive entrance examination, good enough to secure admission. But not good enough for Pasteur. He spent another year on further studies emphasizing physical sciences and then took the École Normale exam again, finishing fourth. That was good enough, and he entered the school in 1843. There he earned his doctoral degree, in physics and chemistry, in 1847.
Among his special interests at the École Normale was crystallography. In particular he was drawn to investigate tartaric acid. It’s a chemical found in grapes responsible for tartar, a potassium compound that collects on the surfaces of wine vats. Scientists had recently discovered that tartaric acid possesses the intriguing power of twisting light — that is, rotating the orientation of light waves’ vibrations. In light that has been polarized (by passing it through certain crystals, filters or some sunglasses), the waves are all aligned in a single plane. Light passing through a tartaric acid solution along one plane emerges in a different plane.
Even more mysteriously, another acid (paratartaric acid, or racemic acid), with the exact same chemical composition as tartaric acid, did not twist light at all. Pasteur found that suspicious. He began a laborious study of the crystals of salts derived from the two acids. He discovered that racemic acid crystals could be sorted into two asymmetric mirror-image shapes, like pairs of right-handed and left-handed gloves. All the tartaric acid crystals, on the other hand, had shapes with identical asymmetry, analogous to gloves that were all right-handed. Pasteur deduced that the asymmetry in the crystals reflected the asymmetric arrangement of atoms in their constituent molecules. Tartaric acid twisted light because of the asymmetry of its molecules, while in racemic acid, the two opposite shapes canceled out each other’s twisting effects.
Pasteur built the rest of his career on this discovery. His research on tartaric acid and wine led eventually to profound realizations about the relationship between microbes and human disease. Before Pasteur, most experts asserted that fermentation was a natural nonbiological chemical process. Yeast, a necessary ingredient in the fermenting fluid, was supposedly a lifeless chemical acting as a catalyst. Pasteur’s experiments showed yeast to be alive, a peculiar kind of “small plant” (now known to be a fungus) that caused fermentation by biological activity.
Pasteur demonstrated that, in the absence of air, yeast acquired oxygen from sugar, converting the sugar to alcohol in the process. “Fermentation by yeast,” he wrote, is “the direct consequence of the processes of nutrition,” a property of a “minute cellular plant … performing its respiratory functions.” Or more succinctly, he proclaimed that “fermentation … is life without air.” (Later scientists found that yeast accomplished fermentation by emitting enzymes that catalyzed the reaction.)
Pasteur also noticed that additional microorganisms present during fermentation could be responsible for the process going awry, a problem threatening the viability of French winemaking and beer brewing. He solved that problem by developing a method of heating that eliminated the bad microorganisms while preserving the quality of the beverages. This method, called “pasteurization,” was later applied to milk, eliminating the threat of illness from drinking milk contaminated by virulent microorganisms. Pasteurization became standard public health practice in the 20th century.
Incorporating additional insights from studies of other forms of fermentation, Pasteur summarized his work on microbial life in a famous paper published in 1857. “This paper can truly be regarded as the beginning of scientific microbiology,” wrote the distinguished microbiologist René Dubos, who called it “one of the most important landmarks of biochemical and biological sciences.”
The germ theory of disease is born Pasteur’s investigations of the growth of microorganisms in fermentation collided with another prominent scientific issue: the possibility of spontaneous generation of life. Popular opinion even among many scientists held that microbial life self-generated under the proper conditions (spoiled meat, for example). Demonstrations by the 17th century Italian scientist Francesco Redi challenged that belief, but the case against spontaneous generation was not airtight. In the early 1860s Pasteur undertook a series of experiments that should have left no doubt that spontaneous generation, under conditions encountered on Earth today, was an illusion. Yet he was nevertheless accosted by critics, such as the French biologist Charles-Philippe Robin, to whom he returned verbal fire. “We trust that the day will come when M. Robin will … acknowledge that he has been in error on the subject of the doctrine of spontaneous generation, which he continues to affirm, without adducing any direct proofs in support of it,” Pasteur remarked.
It was his work on spontaneous generation that led Pasteur directly to the development of the germ theory of disease.
For centuries people had suspected that some diseases must be transmitted from person to person by close contact. But determining exactly how that happened seemed beyond the scope of scientific capabilities. Pasteur, having discerned the role of germs in fermentation, saw instantly that something similar to what made wine go bad might also harm human health.
After disproving spontaneous generation, he realized that there must exist “transmissible, contagious, infectious diseases of which the cause lies essentially and solely in the presence of microscopic organisms.” For some diseases, at least, it was necessary to abandon “the idea of … an infectious element suddenly originating in the bodies of men or animals.” Opinions to the contrary, he wrote, gave rise “to the gratuitous hypothesis of spontaneous generation” and were “fatal to medical progress.”
His first foray into applying the germ theory of disease came during the late 1860s in response to a decline in French silk production because of diseases afflicting silkworms. After success in tackling the silkworms’ maladies, he turned to anthrax, a terrible illness for cattle and humans alike. Many medical experts had long suspected that some form of bacteria caused anthrax, but it was Pasteur’s series of experiments that isolated the responsible microorganism, verifying the germ theory beyond doubt. (Similar work by Robert Koch in Germany around the same time provided further confirmation.)
Understanding anthrax’s cause led to the search for a way to prevent it. In this case, a fortuitous delay in Pasteur’s experiments with cholera in chickens produced a fortunate surprise. In the spring of 1879 he had planned to inject chickens with cholera bacteria he had cultured, but he didn’t get around to it until after his summer vacation. When he injected his chickens in the fall, they unexpectedly failed to get sick. So Pasteur prepared a fresh bacterial culture and brought in a new batch of chickens.
When both the new chickens and the previous batch were given the fresh bacteria, the new ones all died, while nearly all of the original chickens still remained healthy. And so, Pasteur realized, the original culture had weakened in potency over the summer and was unable to cause disease, while the new, obviously potent culture did not harm the chickens previously exposed to the weaker culture. “These animals have been vaccinated,” he declared.
Vaccination, of course, had been invented eight decades earlier, when British physician Edward Jenner protected people from smallpox by first exposing them to cowpox, a similar disease acquired from cows. (Vaccination comes from cowpox’s medical name, vaccinia, from vacca, Latin for cow.) Pasteur realized that the chickens surprisingly displayed a similar instance of vaccination because he was aware of Jenner’s discovery. “Chance favors the prepared mind,” Pasteur was famous for saying.
Because of his work on the germ theory of disease, Pasteur’s mind was prepared to grasp the key role of microbes in the prevention of smallpox, something Jenner could not have known. And Pasteur instantly saw that the specific idea of vaccination for smallpox could be generalized to other diseases. “Instead of depending on the chance finding of naturally occurring immunizing agents, as cowpox was for smallpox,” Dubos observed, “it should be possible to produce vaccines at will in the laboratory.”
Pasteur cultured the anthrax microbe and weakened it for tests in farm animals. Success in such tests not only affirmed the correctness of the germ theory of disease, but also allowed it to gain a foothold in devising new medical practices.
Later Pasteur confronted an even more difficult microscopic foe, the virus that causes rabies. He had begun intense experiments on rabies, a horrifying disease that’s almost always fatal, caused usually by the bites of rabid dogs or other animals. His experiments failed to find any bacterial cause for rabies, leading him to realize that it must be the result of some agent too small to see with his microscope. He could not grow cultures in lab dishes of what he could not see. So instead he decided to grow the disease-causing agent in living tissue — the spinal cords of rabbits. He used dried-out strips of spinal cord from infected rabbits to vaccinate other animals that then survived rabies injections.
Pasteur hesitated to test his rabies treatment on humans. Still, in 1885 when a mother brought to his lab a 9-year-old boy who had been badly bitten by a rabid dog, Pasteur agreed to administer the new vaccine. After a series of injections, the boy recovered fully. Soon more requests came for the rabies vaccine, and by early the next year over 300 rabies patients had received the vaccine and survived, with only one death among them.
Popularly hailed as a hero, Pasteur was also vilified by some hostile doctors, who considered him an uneducated interloper in medicine. Vaccine opponents complained that his vaccine was an untested method that might itself cause death. But of course, critics had also rejected Pasteur’s view of fermentation, the germ theory of disease and his disproof of spontaneous generation. Pasteur stood his ground and eventually prevailed (although he did not turn out to be right about everything). His attitude and legacy of accomplishments inspired 20th century scientists to develop vaccines for more than a dozen deadly diseases. Still more diseases succumbed to antibiotics, following the discovery of penicillin by Alexander Fleming — who declared, “Without Pasteur I would have been nothing.”
Even in Pasteur’s own lifetime, thanks to his defeat of rabies, his public reputation was that of a genius.
Pasteur’s scientific legacy As geniuses go, Pasteur was the opposite of Einstein. To get inspiration for his theories, Einstein imagined riding aside a light beam or daydreamed about falling off a ladder. Pasteur stuck to experiments. He typically initiated his experiments with a suspected result in mind, but he was scrupulous in verifying the conclusions he drew from them. Preconceived ideas, he said, can guide the experimenter’s interrogation of nature but must be abandoned in light of contrary evidence. “The greatest derangement of the mind,” he declared, “is to believe in something because one wishes it to be so.”
So even when Pasteur was sure his view was correct, he insisted on absolute proof, conducting many experiments over and over with variations designed to rule out all but the true interpretation.
“If Pasteur was a genius, it was not through ethereal subtlety of mind,” wrote Pasteur scholar Gerald Geison. Rather, he exhibited “clear-headedness, extraordinary experimental skill and tenacity — almost obstinacy — of purpose.” His tenacity, or obstinacy, helped him persevere through several personal tragedies, such as the deaths of three of his daughters, in 1859, 1865 and 1866. And then in 1868 he suffered a cerebral hemorrhage that left him paralyzed on his left side. But that did not slow his pace or impair continuing his investigations.
“Whatever the circumstances in which he had to work, he never submitted to them, but instead molded them to the demands of his imagination and his will,” Dubos wrote. “He was probably the most dedicated servant that science ever had.”
To the end of his life, Pasteur remained dedicated to science and the scientific method, stressing the importance of experimental science for the benefit of society. Laboratories are “sacred institutions,” he asserted. “Demand that they be multiplied and adorned; they are the temples of wealth and of the future.”
Three years before his death in 1895, Pasteur further extolled the value of science and asserted his optimism that the scientific spirit would prevail. In an address, delivered for him by his son, at a ceremony at the Sorbonne in Paris, he expressed his “invincible belief … that science and peace will triumph over ignorance and war, that nations will unite, not to destroy, but to build, and that the future will belong to those who will have done most for suffering humanity.” Two hundred years after his birth, ignorance and war remain perniciously prominent, as ineradicable as the microbes that continue to threaten public health, with the virus causing COVID-19 the latest conspicuous example. Vaccines, though, have substantially reduced the risks from COVID-19, extending the record of successful vaccines that have already tamed not only smallpox and rabies, but also polio, measles and a host of other once deadly maladies.
Yet even though vaccines have saved countless millions of lives, some politicians and so-called scientists who deny or ignore overwhelming evidence continue to condemn vaccines as more dangerous than the diseases they prevent. True, some vaccines can induce bad reactions, even fatal in a few cases out of millions of vaccinations. But shunning vaccines today, as advocated in artificially amplified social media outrage, is like refusing to eat because some people choke to death on sandwiches.
Today, Pasteur would be vilified just as he was in his own time, probably by some people who don’t even realize that they can safely drink milk because of him. Nobody knows exactly what Pasteur would say to these people now. But it’s certain that he would stand up for truth and science, and would be damn sure to tell everybody to get vaccinated.
Parts of her cultural inheritance are scattered across the Tanami desert in northwestern Australia, where dozens of ancient boab trees are engraved with Aboriginal designs. These tree carvings — called dendroglyphs — could be hundreds or even thousands of years old, yet have received almost no attention from western researchers.
That is slowly starting to change. In the winter of 2021, Garstone — who is Jaru, an Aboriginal group from the Kimberley region of northwestern Australia — teamed up with archaeologists to find and document some of these carvings.
For Garstone, the expedition was a bid to piece back together the disparate parts of her identity. These pieces were scattered 70 years ago when Garstone’s mother and three siblings were among the estimated 100,000 Aboriginal children taken from their families by the Australian government. Like many others, the siblings were sent to live at a Christian mission thousands of kilometers from home. It would take decades of effort and a series of unconnected events — including the gift of an heirloom and a researcher’s quest to find out what happened to a missing 19th century European naturalist — for Garstone’s family to reclaim its birthright. When the siblings returned to their mother’s homeland as teenagers, their extended family gave Garstone’s aunt, Anne Rivers, a coolamon, a type of shallow dish, decorated with two bottle trees, or boabs. Rivers, who was only 2 months old when she was sent away, was told that the trees were a part of her mother’s Dreaming, the cultural story that connected her and her family to the land.
Now, in a study published October 11 in Antiquity, researchers have meticulously described 12 boabs with dendroglyphs in the Tanami desert that have links to Jaru culture. And just in time: The clock is ticking for these ancient engravings as their host trees succumb to the ravages of time and growing pressure from livestock and possibly climate change.
The race to document these engravings before it’s too late isn’t just a matter of studying an ancient art form. It’s also a matter of healing the wounds inflicted by policies intended to erase the connection between Garstone’s family and the land.
“To find evidence that ties us to the land has been amazing,” she says. “The puzzle we’ve been trying to piece together is now complete.”
An outback archive Australian boabs (Adansonia gregorii) proved pivotal to this project. Found in the northwestern corner of Australia, boabs are a species of tree easily recognizable by their massive trunks and iconic bottle shape. Anthropologists have written about the existence of trees carved with Aboriginal symbols in Australia since the early 1900s. These records indicate that people were continuously carving and recarving some trees until at least the 1960s. But compared with other forms of Aboriginal art — such as the visually spectacular paintings also found in the area (SN: 2/5/20) — “there does not appear to be a wide general awareness of this art form,” says Moya Smith, curator of anthropology and archaeology at the Western Australia Museum in Perth, who was not involved with the study.
Darrell Lewis has come across his share of carved boabs. The historian and archaeologist now at the University of New England in Adelaide has worked in the Northern Territory for half a century. Lewis has spotted engravings made by cattle drovers, World War II soldiers and Aboriginal peoples. He calls this eclectic bag of engravings “the outback archive” — a physical testament to the people who have made this rugged part of Australia their home.
In 2008, Lewis was searching the Tanami Desert for what he hoped would be his biggest addition to the archive. He’d heard rumors that a cattle drover working in the area a century earlier had found a firearm stashed in a boab marked with the letter “L.” A roughly cast brass plate from the firearm — later bought by the National Museum of Australia — was stamped with the name of the famed German naturalist Ludwig Leichhardt, who disappeared in 1848 while traveling across western Australia.
The Tanami is generally considered to be outside the boab’s natural range. So in 2007, Lewis rented a helicopter and crisscrossed the desert in search of the Tanami’s secret stash of boabs. His flyovers revealed roughly 280 centuries-old boabs and hundreds of younger trees scattered across the desert.
“Nobody, not even locals, really knew there were any boabs out there,” he recalls. His 2008 ground expedition to find the elusive “L” came up empty-handed. But the search did uncover dozens of boabs marked with dendroglyphs.
In a report for the National Museum of Australia, which had hired him to search for the “L” carving, Lewis recorded the location of these trees. That information sat untouched for years until one day, it fell into the hands of Sue O’Connor, an archaeologist at Australian National University in Canberra.
Crumble into dust In 2018, O’Connor was part of a group of archaeologists who were growing increasingly concerned about the survival of boabs. That year, scientists studying baobabs in Africa — a close relative of boabs — noticed that some of the older trees were dying out at a surprisingly high rate, potentially due to climate change (SN: 6/18/18).
The news alarmed O’Connor. Dendroglyphs are often engraved on the largest and oldest boabs. While nobody knowns exactly how old these trees can get, researchers suspect that their lifetimes could be comparable to their African cousins, which can live up to 2,000 years.
When these long-lived trees do die, they pull a disappearing act. Unlike other trees, whose wood can be preserved for hundreds of years after death, boabs have a moist and fibrous interior that can quickly disintegrate. Lewis has witnessed boabs crumble into the dust a couple of years after being struck by lightning.
“You would never know there’d been a tree there,” he says.
Whether Australian boabs are threatened by climate change is unclear. But the trees are coming under attack from livestock, which peel back boabs’ bark to get to the wet interior. “We put all this together and thought we better try and locate some of the carvings because they probably won’t be there in a few years,” says O’Connor.
Lewis’ report provided a good jumping-off point for this work. So O’Connor reached out to the historian and suggested they collaborate.
Around that same time, Garstone was four years into her own research into her family’s heritage. The long and meandering search led her to a small museum that a friend of Lewis’ happened to run. When Garstone mentioned she was from Halls Creek — a town near where Lewis did his fieldwork in 2008 — the curator told her about the carved boabs.
“I was like, ‘What? That’s a part of our Dreaming!’” she recalls. Dreamings are a western term used to refer to the vast diversity of stories that — among other things — recount how spiritual beings formed the landscape. Dreaming stories also pass down knowledge and inform rules of behavior and social interaction.
Garstone knew from the oral history passed down through her family that her grandmother had ties to the Bottle Tree Dreaming, as indicated by the trees painted on her aunt’s coolamon. The Bottle Tree Dreaming is one of the eastern-most manifestations of the Lingka Dreaming track (Lingka is the Jaru word for the King Brown Snake). This path runs for thousands of kilometers from the western coast of Australia and into the neighboring Northern Territory, marking Lingka’s journey across the landscape and forming a byway for people to travel across the country.
Eager to confirm that the boabs were a part of this Dreaming, Garstone, along with her mother, aunt and a scattering of other family members, joined the archaeologists on their mission to rediscover the boabs.
Into the Tanami On a winter day in 2021, the group set out from the town of Halls Creek and set up camp on a remote pastoral station mainly populated by cattle and feral camels. Every day, the team climbed into all-wheel-drive vehicles and headed out to the last known location of the engraved boabs.
It was hard work. The crew often drove hours to the supposed position of a boab, only to have to stand on top of the vehicles and scan for trees in the distance. What’s more, wooden stakes sticking out of the ground constantly shredded the vehicles’ tires. “We were out there for eight or 10 days,” says O’Connor. “It felt longer.”
The expedition was cut short when they ran out of tires — but not before finding 12 trees with dendroglyphs. To document the finds, the archaeologists took thousands of overlapping pictures, capturing an image of every centimeter of each tree. The team also spotted grinding stones and other tools scattered around the base of the trees. Considering that large boabs provide shade in a desert with little cover, the prevalence of these objects suggests that people probably used the trees as resting spots as well as navigational markers while traveling across the desert, the researchers report in their study.
Some of the carvings on the boabs were of emu and kangaroo tracks. But an overwhelming majority of the engravings were of snakes, some of which undulated across the bark while others coiled onto themselves. The knowledge provided by Garstone and her family, along with historical records from the area, points toward the carvings being linked to the King Brown Snake Dreaming.
“It was surreal,” Garstone says. Seeing the dendroglyphs confirmed the stories passed down in her family and is “pure evidence” of the ancestral connection to country, she says. The rediscovery has been healing, especially for her mother and aunt, both now in their 70s. “All of this was nearly lost because they didn’t grow up in their homeland with their families,” she says.
Maintaining the connection The work to find and document carved boabs in the Tanami and in other parts of the country has just begun. But this initial foray reveals the “vital importance” of scientists working in collaboration with First Nations knowledge holders, says Smith.
O’Connor is organizing another expedition to find the rest of the engravings that Lewis spotted, though she intends to take better wheels or — ideally — a helicopter. Garstone is planning on coming along with more of her extended family in tow.
In the meantime, O’Connor says that their work appears to have stimulated interest among researchers and other Aboriginal groups to rediscover the lost art form and preserve it for future generations.
“Our connection to country is so important to maintain because it makes us who we are as First Nations people,” adds Garstone. “To know that we have a rich cultural heritage and to have our own museum in the bush is something we will treasure forever.”
A recent TV ad features three guys lost in the woods, debating whether they should’ve taken a turn at a pond, which one guy argues is a marsh. “Let’s not pretend you know what a marsh is,” the other snaps. “Could be a bog,” offers the third.
It’s an exchange that probably wouldn’t surprise novelist Annie Proulx. While the various types of peatlands — wetlands rich in partially decayed material called peat — do blend together, I can’t help but think, after reading her latest book, that a historical distaste and underappreciation of wetlands in Western society has led to the average person’s confusion over basic peatland vocabulary.
In Fen, Bog & Swamp: A Short History of Peatland Destruction and Its Role in the Climate Crisis, Proulx seeks to fill the gaps. She details three types of peatland: fens, which are fed by streams and rivers; bogs, fed by rainwater; and swamps, distinguishable by their trees and shrubs. While all three ecosystems are found around most of the world, Proulx focuses primarily on northwestern Europe and North America, where the last few centuries of modern agriculture led to a huge demand for dry land. Wet, muddy and smelly, wetlands were a nightmare for farmers and would-be developers. Since the 1600s, U.S. settlers have drained more than half of the country’s wetlands; just 1 percent of British fens remains today. Only recently have the consequences of these losses become clear. “We are now in the embarrassing position of having to relearn the importance of these strange places,” Proulx writes. For one, peatlands have great ecological value, supporting a variety of wildlife. They also sequester huge amounts of carbon dioxide, and some peatlands prevent shoreline erosion, while buffering land from storm surges (SN: 3/17/18, p. 20). But the book doesn’t spend too much time on nitty-gritty ecology. Instead, Proulx investigates these environments in the context of their relationship with people.
Known for her fiction, Proulx, who penned The Shipping News and “Brokeback Mountain,” draws on historical accounts, literature and archaeological digs to imagine places lost to time. She challenges the notion that wetlands are purely unpleasant or disturbing — think Shrek’s swamp, where only an ogre would want to live, or the Swamps of Sadness in The Neverending Story that swallow up Atreyu’s horse.
Proulx jumps back as far as 20,000 years ago to the bottom of the North Sea, which at the time was a hilly swath called Doggerland. When sea levels rose in the seventh century B.C., people there learned to thrive on the region’s developing fens, hunting for fish and eels. In Ireland, “bog bodies” — many thought to be human sacrifices — have been preserved in the peat for thousands of years; Proulx imagines torchlit ceremonies where people were offered to the mud, a connection to the natural world that is hard for many people to comprehend today. These spaces were integrated into the local cultures, from Renaissance paintings of wetlands to British lingo such as didder (the way a bog quivers when stepped on). Proulx also reflects on her own childhood memories — wandering through wetlands in Connecticut, a swamp in Vermont — and describes how she, like writer Henry David Thoreau, finds beauty in these places. “It is … possible to love a swamp,” she says.
Fens, bogs and swamps are technically distinct, but they’re also fluid; one wetland may transition into another depending on its water source. This same fluidity is reflected in the book, where Proulx flits from one wetland to another, from one part of the world to another, from one millennium to another. At times didactic and meandering, Proulx will veer off to discuss humankind’s destructive tendency not just in wetlands, but nature in general, broadly rehashing aspects of the climate crisis that most readers interested in the environment are probably already familiar with. I was most enthralled — and heartbroken — by the stories I had never heard before: of “Yde Girl,” a redheaded teenager sacrificed to a bog; the zombie fires in Arctic peatlands that burn underground; and the ivory-billed woodpecker, a bird missing from southern U.S. swamps for almost a century.
A newfound treasure trove of ancient fish fossils unearthed in southern China is opening a window into the earliest history of jawed vertebrates — a group that encompasses 99 percent of all living vertebrates on Earth, including humans. The fossil site, dated from 439 million to 436 million years ago, includes a revealing variety of never-before-seen small, toothy, bony fish species.
The diversity of the fossils at this one site not only fills a glaring gap in the fossil record, but also highlights the strangeness that such a gap exists, researchers report in the Sept. 29 Nature.
“These discoveries confirm what we’ve been arguing for” for years, based on smaller bits of fossils, says Michael Coates, a paleobiologist at the University of Chicago who was not involved in the research.
Genetic analyses had previously pointed to this time period, known as the early Silurian Period, as an era of rapid diversification of jawed vertebrates. But the toothy fishes seemed to have left few traces in the fossil record. Instead, as far as the fossil record was concerned, jawless fishes appeared to rule the waves at the time. And what jawed fishes have been preserved were rarely bony; most have been chondrichthyans, ancient cartilaginous ancestors of modern sharks and rays.
The Chongqing Lagerstätte — paleontologists’ word for a rich assemblage of diverse species all preserved together at one site — “fundamentally changes that picture,” write paleontologist You-an Zhu of the Chinese Academy of Sciences in Beijing and colleagues in the study. The site is teeming with toothy, bony fishes, particularly armored placoderms, but bears just one chondrichthyan. The first creatures to develop a backbone were fish, and they did it around 480 million years ago (SN: 10/25/18). Genetic analyses have suggested that by about 450 million years ago, those fish also developed jaws, the better to chomp each other with. But the earliest complete fossils of such jawed fish appear relatively late in the fossil record, about 425 million years ago. By the Devonian Period, which spanned from 419 million to 359 million years ago, jawed fishes were a global phenomenon, earning that era the nickname “Age of Fishes” (SN: 7/17/18).
The discovery also hints that the ancestor of both types of jawed fishes, bony and cartilaginous, could have arisen earlier than thought, Coates says. It’s possible that the last common ancestor of modern jawed vertebrates appeared during the Great Ordovician Biodiversification Event, which began around 471 million years ago (SN: 1/24/17). To date, scientists have found only three varieties of fish body fossils dating to that time period, all jawless, finless and “vaguely resembling a super-sized armor-plated tadpole,” Coates adds.
Here’s a closer look at a few of the newly discovered fishy denizens of the Chongqing Lagerstätte.
Little but fierce About 20 separate specimens of a little fish that the researchers have called Xiushanosteus mirabilis were found at the Chongqing site. Those finds make the animal the most abundant type of fish in that fossil assemblage.
X. mirabilis was only about 30 millimeters long, about the length of a paper clip, but it bears a strong resemblance to larger armored placoderms to come in the future: It had a broad, bony head shield and a body covered in small, diamond-shaped scales. The surprising abundance of this type of fish at a site from the early Silurian Period might just be due to lucky fossilization conditions — the small, delicate bones of X. mirabilis and the other jawed fishes found at Chongqing would be harder to preserve than the larger jawless specimens of the time, or the more robust toothy bony fishes of the later Devonian Period. But another possibility is that this site is an outlier in its time that just happened to be popular with the placoderms.
A heavily armored, diminutive shark Two types of jawed fish arose around 450 million years ago — and both make an appearance at the Chongqing site. The new site is remarkable for its diversity of osteichthyans, bony jawed fishes like X. mirabilis. But cartilaginous Shenacanthus vermiformis also spent some time in this environment.
S. vermiformis is represented by only a single specimen at Chongqing, but like X. mirabilis, it is excellently preserved from head to tail. It was diminutive too, just 22 millimeters long. Though it had a similar body plan to other chondrichthyans, it did differ in one key way: Like X. mirabilis, S. vermiformis was heavily armored, with extensive plates on its underside and back.
A time of transition The Chinese site isn’t just shedding light on ancient jawed fish — it offers a window into the evolutionary transition of body features from jawless to jawed species. One newly discovered jawless creature, dubbed Tujiaaspis vividus, turns out to be closely related to a group of jawed fishes called galeaspids, researchers report in a separate paper in the same issue of Nature.
The well-preserved fossils of T. vividus open up new opportunities to learn how its jawed relatives acquired their arrangements of fins, a transition for which there has been little previous evidence, writes Matt Friedman, a paleontologist at the University of Michigan in Ann Arbor, in a commentary in the same issue of Nature. That’s because galeaspids have distinctive head shields, but scientists haven’t previously been able to peer beneath these fossilized shields to study the hidden anatomy.
Thanks to these close relatives, the researchers pieced together how paired fins in the jawless fish evolved in stages to become separate pectoral and pelvic fins in their jawed cousins. Such fins are the precursors of arms and legs in later tetrapods (SN: 5/30/18).
Scientists have teamed up with tiger sharks to uncover the largest expanse of seagrasses on Earth.
A massive survey of the Bahamas Banks — a cluster of underwater plateaus surrounding the Bahama archipelago — reveals 92,000 square kilometers of seagrasses, marine biologist Oliver Shipley and colleagues report November 1 in Nature Communications. That area is roughly equivalent to half the size of Florida.
The finding expands the estimated global area covered by seagrasses by 41 percent — a potential boon for Earth’s climate, says Shipley, of the Herndon, Va.–based ocean conservation nonprofit Beneath The Waves. Seagrasses can sequester carbon for millennia at rates 35 times faster than tropical rainforests. The newly mapped sea prairie may store 630 million metric tons of carbon, or about a quarter of the carbon trapped by seagrasses worldwide, the team estimates.
Mapping that much seagrass was a colossal task, Shipley says. Guided by previous satellite observations, he and colleagues dove into the sparkling blue waters 2,542 times to survey the meadows up close. The team also recruited eight tiger sharks to aid their efforts. Similar to lions that stalk zebra through tall grasses on the African savanna, the sharks patrol fields of wavy seagrasses for grazing animals to eat (SN: 1/29/18; SN: 5/21/19, SN: 2/16/17).
“We wouldn’t have been able to map anywhere near the extent that we mapped without the help of tiger sharks,” Shipley says.
The team captured the sharks with drumlines and hauled each one onto a boat, mounting a camera and tracking device onto the animal’s back before releasing it. The sharks were typically back in the water in under 10 minutes. The team operated like “a NASCAR pit crew,” Shipley says.
Researchers had previously suggested tracking seagrass-grazing sea turtles and manatees to locate pastures. But tiger sharks were a smart choice because they roam farther and deeper, says Marjolijn Christianen, a marine ecologist at Wageningen University & Research in the Netherlands who was not involved in the new work. “That’s an advantage.” Shipley and colleagues plan to collaborate with other animals — including ocean sunfish — to uncover more submarine meadows (SN: 5/1/15). “With this [approach], the world’s our oyster,” he says.
Fifty years ago, three NASA astronauts splashed down in the Pacific Ocean, concluding the final Apollo mission. Less than a dozen years after President John F. Kennedy challenged the United States to commit itself to “landing a man on the moon and returning him safely back to the Earth,” that historic program had achieved its goals and ended.
Now, we’re going back. But this time will be different.
A pivotal moment for the return of crewed missions to the moon occurred at 1:47 a.m. EST on November 16, with the successful launch of Artemis I. NASA’s high-powered Space Launch System rocket roared and crackled as it lifted off the Florida coast on its maiden voyage. The rocket pushed the Orion capsule toward the moon, on a flight testing the technology that will eventually bring astronauts, both men and women, back to the lunar surface.
“It was just a spectacular launch,” says geologist Jose Hurtado of the University of Texas at El Paso, who works with NASA on mission simulations and programs to train astronauts in geology. “It really hits home to me what I love about space exploration, especially human exploration. It’s just an aspirational and inspirational spectacle, and I hope that everybody that was watching it got some of that inspiration.” Now, the United States and China are leading the way to return humans to the moon. The two countries’ programs are massive and complex undertakings with potentially big payoffs. Both aim to boost scientific understanding about the moon and the early Earth, develop new technologies for space exploration and use on Earth, as well as set the stage for longer-term human space exploration.
Better than rovers Apollo was “a technological program to serve political ends,” says space historian Teasel Muir-Harmony. It was rooted in the political tension and conflict between the United States and the Soviet Union. The program “was about winning the hearts and minds of the world public. It was a demonstration of world leadership … of the strength of democracy and then also of capitalism,” says Muir-Harmony, curator of the Apollo Spacecraft Collection at the Smithsonian National Air and Space Museum in Washington, D.C.
Apollo 11 astronauts Neil Armstrong and Buzz Aldrin took the first-ever steps on the moon on July 20, 1969. Over the next few years, 10 more American men hopped, skipped and even drove across the pewter-colored, lifeless terrain of our planet’s only natural companion. Apollo 17 was the final mission in that series of landings, ending on December 14, 1972 (SN: 12/23/72, p. 404). Once Apollo 17 astronauts Eugene Cernan and Harrison H. Schmitt left their footprints embossed in the lunar dust and joined Ronald Evans in the command module, humans stopped walking on the moon.
In the decades since Apollo 17, about two dozen spacecraft from various countries have visited the moon. Some have orbited, others have slammed into the surface so researchers could study the material in the debris of those collisions, and some have landed and brought lunar samples back to Earth (SN: 1/16/21, p. 7).
While these uncrewed spacecraft have made some big strides in lunar exploration, humans could do better. “Nothing can replace the value of having a human brain and human eyes there on the scene,” Hurtado says. One moment during Apollo 17 makes his point. Schmitt, the only geologist to visit the moon, noticed a patch of lunar soil with a particular rusty hue. He walked over, contemplated the surroundings and realized it was evidence of a volcanic eruption. He and Cernan scooped up some of this orange soil for later Earth-based analyses, which revealed that the orange glass blobs in the soil did in fact form during a “fire fountain” explosion some 3.7 billion years ago.
That discovery supported the idea that the moon had hosted volcanoes in its youth, and additional analysis of the orange soil’s chemical composition hinted that the moon formed at around the same time as Earth. Scientists wouldn’t have had access to the orange soil if it wasn’t for Schmitt’s quick grasp that what he saw was important. “Probably the ultimate field tool is the well-trained human,” Hurtado says.
In his 2005 book, Roving Mars, planetary scientist Steven Squyres wrote: “The unfortunate truth is that most things our rovers can do in a perfect [Martian day], a human explorer on the scene could do in less than a minute.” Squyres, of Cornell University, led the Spirit and Opportunity rover missions to Mars (SN: 8/13/22, p. 20).
A long-awaited lunar return Once Apollo ended, NASA shifted its focus to space stations to prepare for longer-term human spaceflight. Skylab launched in May 1973, hosting four crews of astronauts that year and the next. A few years later, the temporary station broke apart in the atmosphere, as planned. NASA’s next space station, the International Space Station, or ISS, was a larger, collaborative project that’s been hosting astronauts since November 2000. It’s still orbiting roughly 400 kilometers above Earth.
U.S. leaders have occasionally tried to shift NASA’s gaze from low Earth orbit, where the ISS flies, to a more distant frontier. Many presidents have proposed investments in different technology for different exploration goals and with different price tags. But by 2019, the plan was set: NASA would land humans on the moon’s south pole in 2024, though the timeline has since slipped.
“The first woman and the next man on the moon will both be American astronauts, launched by American rockets from American soil,” said Vice President Mike Pence in early 2019. Shortly after, NASA named this effort the Artemis program — after Apollo’s mythological twin sister.
The Artemis program is part of NASA’s Moon to Mars program, which aims to send humans farther into space than ever before. The moon is up first, with astronauts stepping on its surface as early as 2025. What the space agency and its partners learn during a few years of lunar exploration will help guide the phases beyond the moon, including sending astronauts to the Red Planet.
“The goal with Artemis is to build off everything we’ve done to this point and really start to establish a presence for humanity beyond low Earth orbit,” says planetary geologist Jacob Bleacher of NASA’s Human Exploration and Operations Mission Directorate in Washington, D.C.
The first big test for Moon to Mars is to show that NASA’s rocket, the Space Launch System, or SLS, which has been in development for over a decade at a cost of more than $20 billion, can successfully launch a crew capsule, without the crew, beyond low Earth orbit.
But that effort has had a rocky start with the Artemis I launch scrubbed twice for fuel leaks and delayed by two hurricanes. Now that it’s off the ground, Artemis I will test the SLS rocket and the Orion advanced crew capsule on a roughly month-long trip beyond the moon and back (SN: 8/26/22). One more test flight, Artemis II, will follow a similar trajectory as the first mission, but with astronauts on board, launching no earlier than 2024.
Artemis III, slated for 2025, is expected to return boots to the moon and make history by landing the first woman on the lunar surface. On that flight, the SLS rocket will launch the Orion crew capsule toward the moon. When it arrives at lunar orbit, it will dock with the human landing system, currently in development by the company SpaceX. Two astronauts will board the SpaceX vehicle, which will bring them to the moon for a 6.5-day stay. That landing system will also bring the astronauts back to Orion, still in lunar orbit, which will then return them to Earth.
If all goes well, NASA plans to run Artemis missions roughly once a year. “We hope to, through those missions that follow Artemis III, build up some infrastructure,” Bleacher says. That infrastructure will include hardware for developing and distributing power on the moon, rovers for the astronauts to traverse long distances and eventually living and working quarters on the surface. The aim is to increase the astronauts’ length of stay from days to perhaps months.
To help support these lunar astronauts, NASA is leading the creation of a new space station. Called the Gateway, it will orbit the moon when complete, maybe by the 2030s. Like the International Space Station, which is scheduled to safely break apart in early 2031, Gateway will be an international and commercial research station. It will also serve as a way station for trips to Mars and beyond. The moon goddess NASA astronauts likely won’t be the only people exploring the lunar surface. China aims to land its own astronauts at the moon’s south pole by the next decade. Begun in 2004, China’s lunar exploration program, Chang’e — named after the Chinese goddess of the moon — has seen fast progress. It “is very systematic, very well done, and they’ve been successful every step of the way,” says planetary geologist James Head of Brown University in Providence, R.I.
In 2018, China put a relay communication satellite in orbit around the moon. In 2019, China landed a rover on the lunar farside, providing the first up-close view of the side of the moon hidden from Earth. That rover is still operating. In November 2020, China sent another rover, which brought samples from the moon’s nearside to Earth the following month.
Next up, although China doesn’t share its specific schedule plans, is Chang’e 6, which will collect and return material from the moon’s farside. In 2026, China intends to launch its Chang’e 7 mission to the south pole to search for water ice. “There’s no question,” Head says, “that [China] will be sending humans to the moon toward the end of the decade.”
China’s human-occupied space station, called Tiangong, is now complete and in low Earth orbit. And Mars exploration is on the menu as well. China landed a rover safely there in 2021 and is gearing up for a sample-return mission in the same time frame as a NASA-European Space Agency sample-return mission to Mars. Science is an international endeavor, but NASA and China’s space agency are unable to collaborate due to the Wolf Amendment (SN: 11/24/18, p. 14). Tacked onto a U.S. appropriations bill in 2011, the amendment prohibits NASA and the White House Office of Science and Technology Policy from collaborating, designing and planning projects with China, unless authorization is granted by the U.S. Congress.
Some lunar scientists, however, hope there can be collaboration between the two nations, such as sharing returned samples. “There are a lot of different places to go in space, and there’s no sense duplicating everything,” Head says.
While human space exploration began as a competition, international collaboration is now the norm. Astronauts from 20 countries have visited the International Space Station over its 22-year history, living together for months and working toward shared interests.
“The International Space Station is a frigging United Nations in orbit in a tin can,” Head says. Private firms also have become increasingly involved in the ISS. And for the Moon to Mars program, international space agencies and private companies are participating, designing and fabricating crucial components. To the south pole When humans step on the moon again, they’ll investigate a never-before-explored locale, the moon’s south pole. It’s a region rich with impact craters, uplifted ancient material and water ice (SN: 11/13/09). Both the United States and China are targeting this area to answer new research questions and to access resources humans would need for an extended stay.
This cratered terrain reveals when rocky material tore through the solar system in the first billion years of its history, slamming into the nascent planets (SN: 4/25/12). Earth no longer tells that history, but the moon, without liquid water or a robust atmosphere to smooth away the evidence, retains a surface record of meteorite impacts over billions of years. “Because that record is so perfectly preserved on the lunar surface, it is the single best place in the entire solar system to understand the origin and early evolution of planets,” says planetary scientist David Kring of the Lunar and Planetary Institute in Houston.
And while those are important mysteries, the south pole’s deep craters also hold something thrilling — water ice. There’s a lot to learn about that ice, says lunar exploration scientist Clive Neal of the University of Notre Dame in Indiana. How much is there? Can it be extracted? How to refine it for human use? The Artemis explorers can address those questions, which would enable even longer-term exploration.
That’s the goal this time around: to stay longer for both science exploration and to learn how humans can have a lasting presence on another celestial body. This work “would extend the bounds of human experience in a way that has never happened before,” the Smithsonian’s Muir-Harmony says.
That’s a tall order, considering how NASA’s schedules keep slipping and the cost estimates for each piece of Moon to Mars keep ballooning. A 2021 audit estimates that by the end of 2025, the cost for the Artemis program will reach $93 billion, some $25 billion over NASA estimates.
These next few years of Artemis flights will show what NASA can do. And China’s upcoming missions will show what that nation’s lunar exploration can achieve. The world will be watching both.
SAN DIEGO — Scientists have devised ways to “read” words directly from brains. Brain implants can translate internal speech into external signals, permitting communication from people with paralysis or other diseases that steal their ability to talk or type.
New results from two studies, presented November 13 at the annual meeting of the Society for Neuroscience, “provide additional evidence of the extraordinary potential” that brain implants have for restoring lost communication, says neuroscientist and neurocritical care physician Leigh Hochberg.
Some people who need help communicating can currently use devices that require small movements, such as eye gaze changes. Those tasks aren’t possible for everyone. So the new studies targeted internal speech, which requires a person to do nothing more than think.
“Our device predicts internal speech directly, allowing the patient to just focus on saying a word inside their head and transform it into text,” says Sarah Wandelt, a neuroscientist at Caltech. Internal speech “could be much simpler and more intuitive than requiring the patient to spell out words or mouth them.”
Neural signals associated with words are detected by electrodes implanted in the brain. The signals can then be translated into text, which can be made audible by computer programs that generate speech.
That approach is “really exciting, and reinforces the power of bringing together fundamental neuroscience, neuroengineering and machine learning approaches for the restoration of communication and mobility,” says Hochberg, of Massachusetts General Hospital and Harvard Medical School in Boston, and Brown University in Providence, R.I.
Wandelt and colleagues could accurately predict which of eight words a person who was paralyzed below the neck was thinking. The man was bilingual, and the researchers could detect both English and Spanish words.
Electrodes picked up nerve cell signals in his posterior parietal cortex, a brain area involved in speech and hand movements. A brain implant there might eventually be used to control devices that can perform tasks usually done by a hand too, Wandelt says.
Another approach, led by neuroscientist Sean Metzger of the University of California, San Francisco and his colleagues, relied on spelling. The participant was a man called Pancho who hadn’t been able to speak for more than 15 years after a car accident and stroke. In the new study, Pancho didn’t use letters; instead, he attempted to silently say code words, such as “alpha” for A and “echo” for E.
By stringing these code letters into words, the man produced sentences such as “I do not want that” and “You have got to be kidding.” Each spelling session would end when the man attempted to squeeze his hand, thereby creating a movement-related neural signal that would stop the decoding. These results presented at the neuroscience meeting were also published November 8 in Nature Communications.
This system allowed Pancho to produce around seven words per minute. That’s faster than the roughly five words per minute his current communication device can make, but much slower than normal speech, typically about 150 words a minute. “That’s the speed we’d love to hit one day,” Metzger says.
To be useful, the current techniques will need to get faster and more accurate. It’s also unclear whether the technology will work for other people, perhaps with more profound speech disorders. “These are still early days for the technologies,” Hochberg says.
Progress will be possible only with the help of people who volunteer for the studies. “The field will continue to benefit from the incredible people who enroll in clinical trials,” says Hochberg, “as their participation is absolutely vital to the successful translation of these early findings into clinical utility.”
Daylight saving time has ended, and most Americans have turned their clocks back an hour. My sixth-grader is in heaven.
At 6:50 a.m. these days, our once testy tween zombie is now … moderately awake and relatively lucid.
Instead of rising to gauzy predawn light, she’s got glowy morning sunshine beaming around her curtains. When she sets off for school, the sun has been up nearly a full hour. Just a 60-minute change has lightened both the morning and her mood. At breakfast today, I think I even spied a smile.
On November 6, every state in the United States except Hawaii and most of Arizona switched from daylight saving time, or DST, to standard time (those two states don’t observe DST). That switch shifted an hour of light from the evening to the morning. In March, we’ll move in the other direction when we “spring forward,” trading morning light for brighter evenings.
The United States’ biannual time change has been lighting up headlines since the U.S. Senate’s unanimous vote in March to make daylight saving time permanent. The Sunshine Protection Act would forgo turning clocks to and fro, repeating an unpopular experiment Congress tried in the 1970s and prioritizing evening light throughout the year. But the health case for staying on daylight saving time is pretty dim. And what such a shift could mean for adolescents is especially gloomy.
Even the name “daylight saving time” isn’t quite right, says Kenneth Wright, a sleep and circadian expert at the University of Colorado Boulder. There’s no change in the amount of daylight, he says. “What we’re doing is changing how we live relative to the sun.” When we move our clocks forward an hour, noon no longer represents when the sun is near its highest point in the sky. Suddenly, people’s schedules are solarly out of sync (SN: 10/17/16).
That’s a big deal biologically, Wright says. Humans evolved with a daily cycle of light and dark. That sets the rhythms of our bodies, from when we sleep and wake to when hormones are released. Morning light, in particular, is a key wake-up signal. When we tinker with time, he says, “we’re essentially making the choice: Do we want to go with what we’ve evolved with, or do we want to alter that?”
From a health perspective, if he had to rank permanent daylight saving time, permanent standard time or our current practice of biannual clock changing, Wright says, “I think the answer is incredibly clear.” Permanent standard time is healthiest for humans, he says. In his view, permanent daylight saving time ranks last.
Daylight saving time takes a toll on health Wright is not alone. As daylight saving time ticked toward its yearly end, sleep experts across the country stepped out in favor of standard time.
Scientists have linked sleep loss, heart attacks and an increased risk of dying in the hospital after a stroke to the transition to daylight saving time, neurologist Beth Malow wrote in Sleep in September. She testified to that this year before a U.S. House of Representatives subcommittee.
“My overall message was that permanent standard time was a healthier choice,” says Malow, of Vanderbilt University Medical Center in Nashville.
For both Malow and Wright, some of the most compelling studies examine U.S. time zone borders. Living on the late sunset side of a border takes a toll on people’s health and sleep compared with those living on the early sunset side, scientists suggested in 2019. A similar study in 2018 also found an increased risk of liver cancer the farther west people lived within a time zone, where the sun rises and sets later in the day.
But the downsides of nighttime light are not always crystal clear. A November study, for example, suggested that year-round daylight saving time would reduce deer-vehicle collisions (SN: 11/2/22). But studies like these can be hard to interpret, Malow says. Other factors may come into play, like deer’s seasonal activity and changing roadway conditions. “The car-crash literature has been so mixed,” she says. “I’ve seen stuff come out on both sides.”
She points to a study in Time & Society in June which found that people on the western edge of a time zone had more automobile fatalities than their easterly neighbors.
Dark mornings and light evenings mean people’s body clocks don’t line up with the sun. That mismatch can hamper sleep, making for drowsy drivers, which may factor into collisions, Malow says. In the evenings, if “there’s still light in the sky, it messes with our brains.” Morning light wakes up the brain The brains of teens and tweens are even more vulnerable, Malow says. When kids go through puberty, the brain waits an hour or two longer to release melatonin, the “hormone of darkness,” which tells the bodies of kids and adults alike that it’s time to go to sleep.
Bedtime can be tough for older kids because, physiologically, they’re just not as sleepy as they used to be. And as I’ve learned with my daughter, if you throw early school start times in the mix, rising and shining can be even harder.
“I have a middle schooler, too. It’s brutal,” says Lisa Meltzer, a pediatric sleep psychologist at National Jewish Health in Denver. Some U.S. school districts are making changes that might make mornings easier. This year, most high schools and middle schools in California debuted later start times. Five years ago, Meltzer’s school district embarked on a similar experiment. What they learned can teach us how older kids might fare if daylight saving time were to stay put year-round, Meltzer says.
In 2017, the Cherry Creek School District in suburban Denver flipped middle and high schools’ early start times with elementary schools’ later ones. The change didn’t much affect younger kids, who still started class well after sunrise, at 8 a.m., says Meltzer, who presented the science behind changing school start times to her school board. But older kids, who started school at 8:20 a.m. or 8:50 a.m., noticed a big difference. They slept more at night and tended to function better during the day, Meltzer’s team reported most recently in the February Sleep Medicine.
“The number one thing [high-schoolers] said was how much they liked going to school when it was light out,” she says.
And it wasn’t just the students. Their teachers, too, felt the benefits of later start times, Meltzer and colleagues report November 6 in the Journal of School Health.
Morning light is crucial for keeping people’s bodies on schedule, Meltzer says. With permanent daylight saving time, kids will not have the same eye-opening, brain-wakening, a.m. sunshine. “We need morning sunlight to keep our internal clocks on track,” she says. “I cannot emphasize this enough.”
So far, the Senate’s plan for year-round daylight saving time has seemed to stall, so the prospect of an everlasting shift toward evening light doesn’t look bright. But come March, when daylight saving time begins anew, we’ll have to adjust again.
For kids struggling with sleep, Sonal Malhotra, a pediatric pulmonologist and sleep doctor at Baylor College of Medicine in Houston, has some tips. Consistency is key, she says: regular sleep, meal and exercise schedules. And when waking up, she adds, “make sure you have bright light.” Malhotra also recommends avoiding afternoon naps and caffeine.
I don’t know if my daughter will ever be bright-eyed and bushy-tailed in the mornings (I’m not), but when mornings eventually get darker, Malhotra’s advice may give us something to fall back on.
You don’t need a dandelion to know which way the wind blows. But it can help.
On any given dandelion, some seeds are destined to go north, while others are fated to fly east, south or west, and every direction in between. In effect, each dandelion seed is programmed to release for a wind coming from one direction and resists winds from other directions, according to research to be presented at the American Physical Society’s Division of Fluid Dynamics in Indianapolis on November 20.
Dandelion seeds are susceptible to different wind directions depending on where they are on the seed head, says Jena Shields, a biophysicist at Cornell University. The feathery seeds on the side facing a breeze will let go most easily; the others hold on tens to hundreds of times tighter — until the wind shifts. It’s a phenomenon that Shields set out to study after her adviser noticed the way dandelions responded as his toddler played with the flowers.
Shields measured the force it takes to pluck dandelion seeds by supergluing a fine wire to the tufted ends and pulling them from the seed heads at various angles. This seed-by-seed study mimicked what happens when wind, or a child’s breath, pushes them over. Because each seed is most susceptible to winds from distinct directions, it helps prevent seeds from all going the same way, Shields says, and may explain why the plants are so successful at spreading. Once blown off a dandelion, the umbrella-like tuft on a seed carries it on the breeze that pulled it away (SN: 10/17/18).
“But a strong, turbulent wind can still send all the seeds flying in the same direction,” Shields says, so the effect can’t guarantee that a powerful gust or exuberant child won’t blow off all the seeds at once.